

T.K. is 5 years old but weighs only about 8 kg—small like a one-year-old infant—with cyanotic lips and a chest visibly heaving with labored breathing. This abnormal physical condition became the first clue that helped doctors at the Heart Center, Vietnam National Children’s Hospital diagnose a complex congenital heart defect. From that moment, a race against time began: bringing the child from a highland village in Lai Chau to Hanoi and performing emergency surgery in less than 24 hours to give him a chance at survival.

The patient returned for follow-up after surgery.
Five years living with a congenital heart defect—without anyone knowing
Born into a farming family in Pac Ta Commune (Lai Chau), T.K. had been underweight and growing more slowly than peers since early childhood. He frequently experienced shortness of breath, bluish discoloration of the lips and fingernails, and poor appetite; however, the family attributed these symptoms to malnutrition or a weak constitution.
What no one realized was that for five years, T.K. had been living with one of the most dangerous congenital heart defects: obstructed anomalous pulmonary venous return—a condition that causes severe lung damage, and in which most children have little chance of survival if not diagnosed and surgically treated promptly during the neonatal period.

Although nearly 5 years old, T.K. weighed only about 8 kg.
T.K.’s condition was discovered incidentally during the free screening program “Hearts for Children” in Lai Chau, held over two days (11–12 April 2026).
An urgent persuasion effort in a remote village
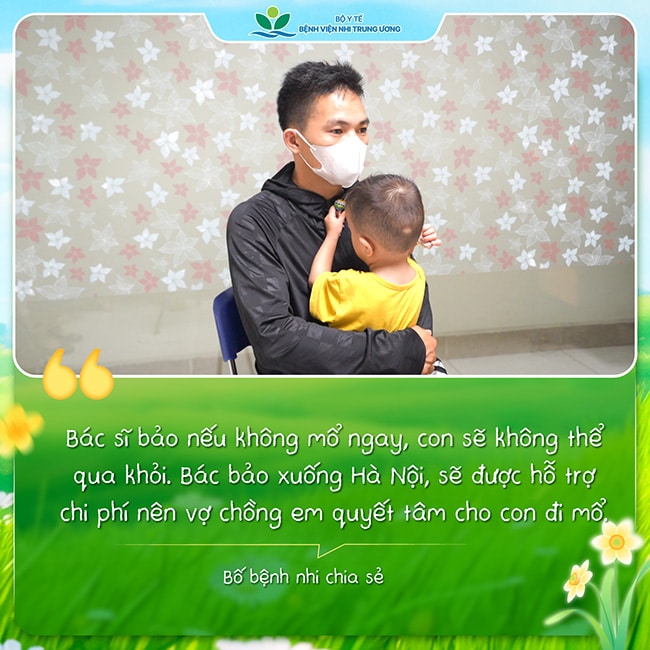
Hearing that their child had a life-threatening heart condition left the family devastated. For people whose lives revolved around fields and farming, Hanoi felt impossibly far away, and heart surgery was beyond imagination. It was not only fear of illness, but also anxiety about costs, the long journey, and the child’s fragile chance of survival.
Understanding the family’s circumstances, immediately after the screening on the morning of 11/04/2026, Assoc. Prof. Nguyen Ly Thinh Truong, MD, PhD, traveled more than two hours along mountainous roads to the village, coordinating with local authorities to persuade the family to bring the child to Hanoi for treatment. Surgical and living costs would be supported by the national health insurance fund together with the “Hearts for Children” program.
At around 3:00 p.m. that same day, a special vehicle departed Lai Chau, traveling more than 300 km through mountain passes and arriving at Vietnam National Children’s Hospital at 8:30 p.m. in an extremely urgent context—because the child could deteriorate at any time during transport.

At Vietnam National Children’s Hospital, the child was rapidly evaluated and underwent advanced investigations.
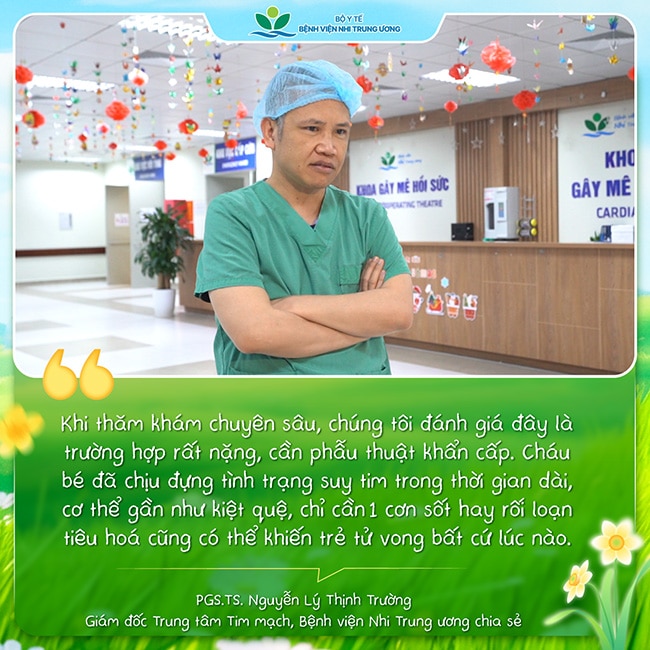
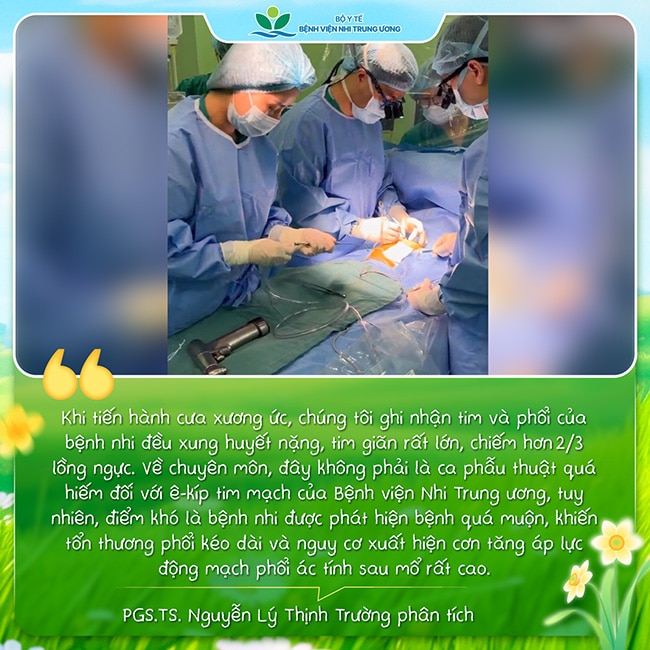
A massively enlarged heart occupying more than two-thirds of the chest—and emergency surgery within 24 hours
“At the time of admission, the child had New York Heart Association (NYHA) class III heart failure, severe malnutrition, and severe lung injury. Remarkably, surviving to 5 years of age with this condition is extremely rare—well beyond the usual prognosis. Fortunately, despite the critical severity, the lungs still had recovery potential, so we decided to operate in the hope of saving the child,” Assoc. Prof. Nguyen Ly Thinh Truong shared.
The next morning, T.K. underwent emergency surgery. The surgical team redirected the pulmonary veins back to their normal anatomical position.
After surgery, the challenges were not over
The greatest challenge was not only in the operating room, but also in the postoperative period, as the child’s lungs had suffered long-standing injury, beginning to develop fibrosis and facing the risk of malignant pulmonary hypertension—a complication that can be fatal within a short time.
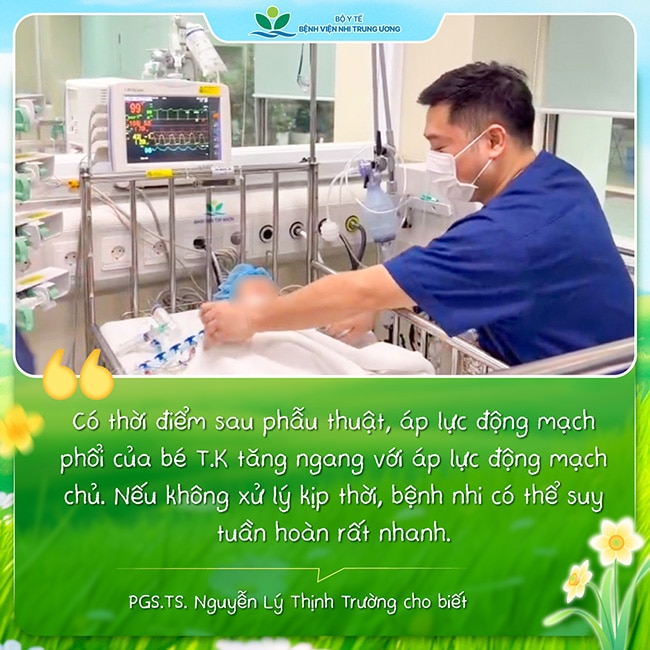
In Viet Nam, treating postoperative pulmonary arterial hypertension remains challenging due to limited availability of nitric oxide delivery systems, an important supportive therapy in many high-income settings. Therefore, doctors had to continuously monitor pulmonary arterial pressure and implement multiple measures to control it.
A life regained after a near-fatal journey
After nearly five days of intensive care, T.K. was weaned from mechanical ventilation. Encouragingly, the child responded to treatment better than expected. Although the lungs had previously been injured, cardiac function is now close to normal.
“Before, we only hoped our child would survive. Now, seeing our child become healthier every day, our whole family feels like our child has been born a second time,” the father said emotionally.
Do not overlook warning signs: poor weight gain, rapid breathing, cyanosis
Pulmonary venous anomalies can be difficult to detect during pregnancy and require highly experienced fetal echocardiography. After birth, about 80% of children show cyanosis and are more easily detected; however, the remaining 20% may not be cyanotic and are therefore often diagnosed late. If detected and treated early, survival chances are high. In contrast, delayed diagnosis leads to severe lung damage and significantly reduced survival.
Assoc. Prof. Nguyen Ly Thinh Truong emphasized that parents should pay close attention to warning signs of severe congenital heart disease requiring early detection, including poor weight gain, poor feeding, tachypnea, cyanosis, excessive sweating, or recurrent pneumonia. When such signs are suspected, children should be brought promptly to specialized cardiology centers for timely evaluation and treatment.

The child’s hand appears pink and well-perfused after recovery.
Over the past 15 years, the Heart Center, Vietnam National Children’s Hospital, has performed surgery for more than 500 children with pulmonary venous anomalies (a record in Southeast Asia), with an early survival rate of nearly 94%, comparable to major cardiac centers worldwide. The lowest body weight successfully operated on was 1.8 kg. Many children have undergone emergency surgery just hours after birth—offering survival to hundreds of young hearts that once seemed to have no hope.
Digital Information Office – Training and Research Institute for Child Health
